

The Fifth Wave: When Medicine Stops Waiting for Disease
Medicine has stopped resisting AI. The next leap in healthy human lifespan is closer than the institutions admit.

Issue #52 | Week 19 | Sunday 3 May 2026
This issue is also available as a podcast. Listen on Spotify, Apple Podcasts or YouTube and tell me what you think.
The Bottom Line Up Front
Healthcare is the most regulated, slowest-moving and institutionally defended industry in the modern economy. This week, all three of those defences cracked in the same direction.
The Food and Drug Administration, an agency whose clinical trial review architecture has not meaningfully changed since the 1960s, announced it will use artificial intelligence to monitor drug trials in real time. AstraZeneca and Amgen are already named as proof-of-concept partners. The FDA’s own Commissioner concedes that forty per cent of clinical trial time is “dead time” that AI will dissolve.
That is not an efficiency programme. It is a regime change.
It is happening at exactly the moment when individuals like me have stopped waiting for the NHS to catch up and started building our own AI health systems from Whoop data, blood panels and personal medical records.
This issue is about what happens when the floor under medicine starts to move. Three stories. The regulator. The patient. And the prize at the end of all this. The first credible challenge to the limits of healthy human lifespan in a hundred years.
The Tech Layoff Tracker, now in its twentieth week, also crossed an inflection point. The polite fiction of “AI-assisted workforces” is starting to break. Cloudflare cut twenty per cent. Coinbase, Freshworks, Upwork and BILL Holdings followed. The euphemism this week was “agentic AI-first.” The reality was the same.
Let’s get into it.
1. The Compression of Medical Time
The FDA broke the bottleneck. The rest of medicine is about to follow.
For sixty years, getting a drug from the laboratory bench to the patient bedside has taken between ten and twelve years. Of that, roughly half is what FDA Commissioner Marty Makary now publicly calls “dead time.” Paperwork. Data entry. Months in which trials sit idle while files move from a sponsor to a regulator who has not seen them.

On 28 April 2026, the FDA announced the first serious attempt to end this.
The agency’s new Real-Time Clinical Trials pilot, run by Chief AI Officer Jeremy Walsh, allows FDA reviewers direct access to clinical trial data the moment it is generated. AstraZeneca and Amgen are already involved in the proof-of-concept phase, both with cancer drugs. Walsh estimates the pilot could remove twenty to forty per cent of total clinical trial time. The agency is also accepting public comment on a broader pilot for AI in early-phase trials until the end of May.
This was paired with an even bigger move. The FDA’s own internal AI tool, Elsa, deployed in June 2025 to accelerate scientific review, has now been integrated with a consolidated data platform across the entire agency. The savings from system consolidation are being reinvested in onboarding thousands of FDA staff and contractors, including scientific reviewers.
Read those two paragraphs again. The most cautious regulator in the developed world has just compressed its own review architecture using artificial intelligence, then turned that architecture outward to compress the trials themselves.
This is what my Yorkshire Post column explores in detail this week, under the title Britain can lead the way in AI-powered medical advances. The story is not that AI is invading medicine. The story is that medicine’s gatekeepers have stopped resisting.
A drug development pathway that has historically taken ten to twelve years may, by the end of this decade, lose years of dead time. Not because biology becomes simple, but because paperwork, handoffs and regulatory latency finally become machine-readable.
Britain has movement, but not yet the same symbolic rupture. The MHRA and HRA have just introduced the largest package of clinical trial reforms in more than twenty years, including faster assessment of first-in-human trials, lower-risk notifiable trials, and recognition of computer modelling. The MHRA has also expanded AI Airlock, its regulatory sandbox for AI as a medical device. But none of this yet matches the FDA’s central leap: giving reviewers real-time access to live trial signals and using AI to compress the trial architecture itself. That is the gap. And capital notices gaps.
The FDA initiative has critics. Elsa, the agency’s internal AI tool, has been accused of hallucinating false information. The Commissioner’s National Priority Voucher programme has faced corruption concerns. Layoffs and political interference at the FDA continue to draw scrutiny. None of that changes the direction of travel. Real-time monitoring. Pilot programmes with major pharma. An AI officer with executive authority to set the agenda.
Britain is watching another regulator move first. Again.
2. The Patient Builds the Model
Two years ago I sat in an A&E corridor with my AI in my pocket. This year I built my own.
Some of you will remember an earlier column where I wrote about taking a family member into hospital with suspected stroke symptoms. The full version was published in the Yorkshire Post at the time. The short version: I sat in a corridor for hours, watching exhausted clinicians work through a queue that had no end, and I used a large language model on my laptop to think through what questions to ask, what red flags to watch for, what the likely differential diagnoses were given the presenting symptoms.

It did not replace the doctor. It made me a better advocate for the person I had brought in.
That experience changed how I think about medicine. Not because the AI was infallible. It was not. But because in the gap between a clinician’s available attention and the speed of a deteriorating patient, there is a space that AI fills usefully and clinicians simply cannot.
Two years on, I have gone further. I have built a personal AI health model on my own data. It has my Whoop biometric stream, every night and every morning. Resting heart rate. Heart rate variability. Sleep stages. Recovery scores. It has the full set of blood panels I have run privately. It has every NHS record I have been able to obtain on myself. It runs continuously, looking for patterns, flagging shifts, suggesting questions for my next consultation.
It is not a substitute for a doctor. It is the health assistant I would have hired if such a role existed.
Why did I build it? Because primary care, in both the United States and the United Kingdom, has missed things. Anyone who has had any serious engagement with primary care in either system over the last decade has at least one story of a missed signal, a delayed referral, a flag that should have been raised months earlier. This is not a criticism of any individual doctor. The professionals I have dealt with have been overwhelmingly diligent.
The system that asks them to evaluate a multi-decade health history in eight minutes is the problem.
AI does not have an eight-minute limit. It does not get tired. It does not lose track of which patient said which thing on which visit. It can hold the whole picture, all the time, and surface the bit that matters today.
The NHS knows this. The Department of Health published an AI Diagnostic Fund of twenty-one million pounds in 2023 to deploy AI imaging tools in stroke and cancer pathways. The NHS Confederation continues to point at AI as the most likely route to relieve administrative pressure on staff. There are pilots running in mental health, dermatology, and radiology. But the gap between pilot and rollout is years. Patients live and die in that gap.
The question is not whether AI will be used by virtually everyone in the NHS. It will. The question is whether we are willing to wait for institutional adoption before benefiting from what is already possible, individually, today.
I was not willing to wait. I built my own. More and more people will do the same.
The hard question is not whether patients will build these systems. They will. The hard question is whether we build the secure, auditable, clinically bounded infrastructure that allows them to do it safely. A personal health model connected to wearables, blood panels and medical records is powerful. It is also sensitive, private and potentially dangerous if treated as a doctor rather than an advocate. That distinction matters.
3. The Fifth Wave
For two centuries, medicine fought the elements. The next wave fights biology itself.
Step back from the news cycle for a moment.
The single greatest achievement in human history is not the moon landing, not the internet, not the printing press. It is the doubling of human life expectancy.
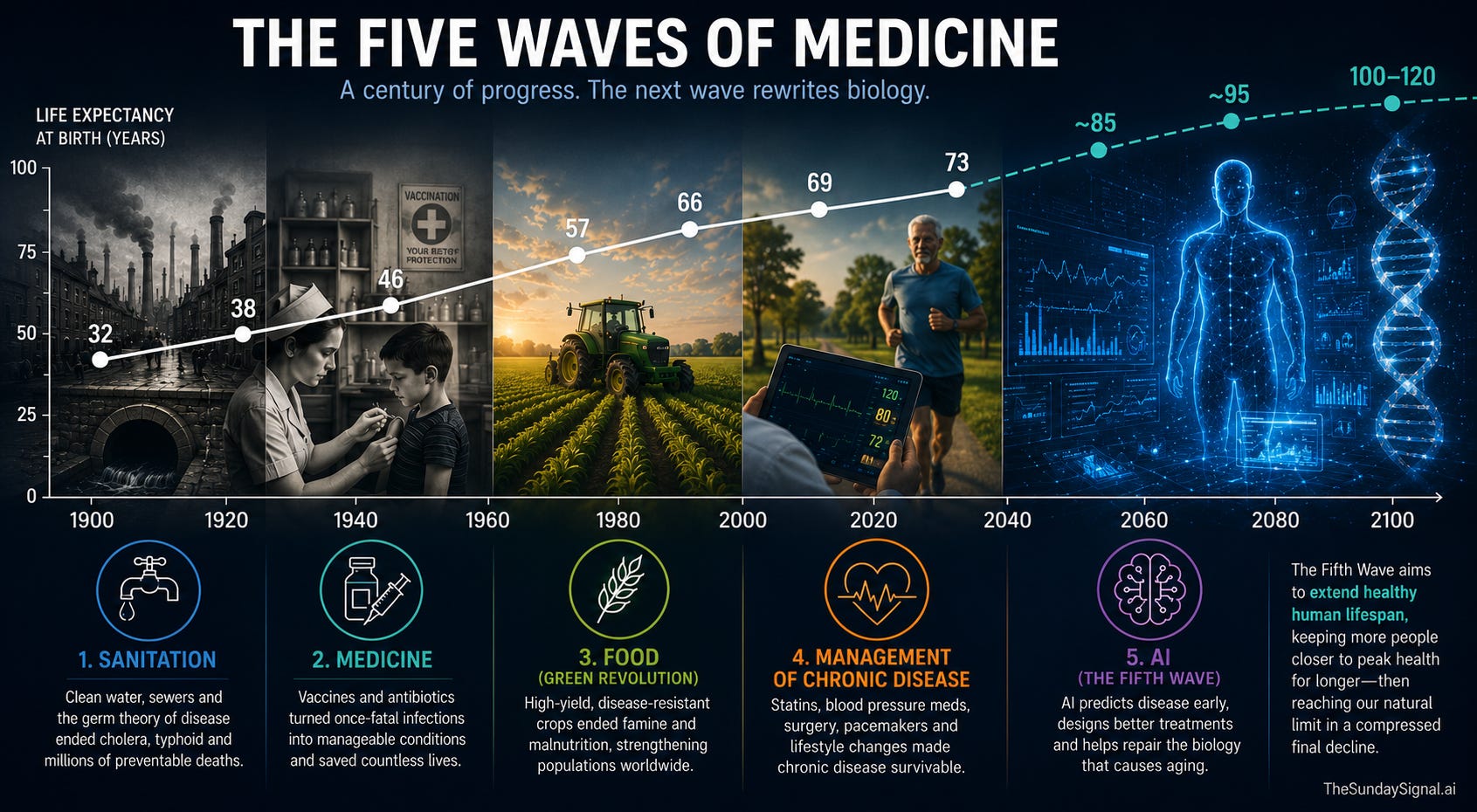
In 1900, global average life expectancy at birth was around thirty-two years. The latest global data puts it at around seventy-three. Across the developed world it is over eighty. We did this in just over a century. No previous society achieved anything comparable. The doubling rests on four waves of breakthrough that arrived in sequence.
The first wave was sanitation. London’s sewers, water chlorination, the germ theory of disease. We stopped living in our own waste and stopped dying of cholera and typhoid in the millions.
The second wave was the golden age of medicine. Vaccines for smallpox, polio, measles. Antibiotics from Fleming’s penicillin onward. A simple scratch stopped being a death sentence.
The third wave was the Green Revolution. Norman Borlaug’s high-yield disease-resistant crops. Famine retreated. Malnutrition stopped weakening immune systems on a population scale.
The fourth wave was chronic disease management. Statins. Blood pressure medication. Bypass surgery. Pacemakers. The collapse of smoking rates. Heart disease became survivable.
Each wave delayed when, and how, the human body collapsed. None of them stopped the collapse itself. For the past twenty years, the curve has flattened. We have run out of low-hanging fruit. Treating Alzheimer’s, late-stage cancer, or heart failure in an eighty-year-old is biological whack-a-mole. Cure one and another arrives, because the underlying machinery is degrading.
Here is the case for the fifth wave: medicine stops waiting for symptoms and starts engineering around biological failure before it happens.
For the first time, medicine is moving from a reactive, observational science into a predictive engineering discipline. AI ingests genomic data, continuous wearable biometrics, and full electronic health records, then finds the microscopic footprint of disease years before symptoms appear. Researchers at the European Molecular Biology Laboratory deployed a generative AI in late 2025 that synthesises individual data to predict risk for over a thousand diseases. UC San Diego used AI to find that the gene PHGDH does not just mark Alzheimer’s, it causes it. The Mayo Clinic Platform now supports cohort identification, AI model development, and real-world evidence generation across multiple institutions on de-identified data.
Drug discovery, historically a scavenger hunt for molecules in mould and bark, is now a programming problem. AlphaFold-class models, and the new generation of agentic biological AI like Google’s Gemini co-scientist, design novel proteins that have never existed in nature. The timeline from biological insight to testable drug is collapsing from a decade to weeks of computational design.
And, most ambitiously, AI is mapping the regulatory networks of the cell. The mechanisms of cellular senescence and epigenetic degradation, the actual code of biological aging, are being identified by AI running millions of simulated experiments. We are moving from treating the symptoms of aging to patching the code of aging.
What does this mean for healthy lifespan?
Dario Amodei, the chief executive of Anthropic, has argued in his essay Machines of Loving Grace that AI could compress a century of biomedical progress into five to ten years and push human life expectancy toward 150. The Silicon Valley version of the fifth wave is utopian. It is also wrong on timeline.
The reason it is wrong is biology, not software. An AI can design a molecular cure for cellular aging in three seconds on a server. It cannot run a ten-year longitudinal aging trial in three seconds. You still have to give the drug to a human, wait, and see whether they aged slower or developed catastrophic tumours. Even with the FDA’s compression of clinical trial time, you cannot fast-forward physical biological decay. The “in silico” cure does not equal the “in vivo” cure.
What is realistic is something closer to the squaring of the mortality curve. Today, human health declines steadily from middle age until death. The fifth wave may allow more people to stay closer to peak biological capacity for decades longer, then collapse fast at the absolute biological maximum, somewhere between 100 and 120. The triumph is not 150-year-old humans by 2036. The triumph is most of the population reaching their natural ceiling in vigorous health, then dying compressed rather than dying slowly.
That is the real prize. It is also the prize that the FDA’s regime change, and the personal AI models patients are now building, are bringing forward by years.
The fifth wave is here. The institutions that build for it now will define the next century of medicine. The institutions that wait will be left explaining why.
The Sunday Signal Tech & AI Layoff Tracker
Issue #53 | Week 20 | Reporting on 3–9 May 2026

The Signal: The “AI-Native” Pivot Stops Pretending
In previous weeks we tracked what I have been calling the “AI Launder”: executives using AI as a PR shield for traditional, macroeconomic cost-cutting. This week, that fig leaf was discarded entirely.
Companies are no longer trimming. They are dissolving departments that cannot be rebuilt on an autonomous foundation. The message from the C-suite is now explicit: if your team is a wrapper around a process that an AI agent can perform natively, that team no longer has a seat at the table.
We are moving from AI-assisted workforces to AI-first architectures. The mid-cap sector is leading the purge.
The Twin Pillars: Cloudflare and Coinbase
Cloudflare announced 1,100 cuts on 7 May, roughly twenty per cent of its 5,500 workforce. This is the case study of the quarter. Co-founder and CEO Matthew Prince told the earnings call that internal AI usage at Cloudflare had risen by more than six hundred per cent in three months. He framed the cuts not as cost-cutting but as defining “how a world-class, high-growth company operates and creates value in the agentic AI era.” Severance is unusually generous: full base pay through year-end, equity vesting extended to August, immigration support for visa-dependent staff. Stock fell 24 per cent the next day despite a Q1 revenue beat.
Coinbase confirmed a restructuring impacting around 700 workers (roughly fourteen per cent) on 5 May. The company cited both AI productivity gains and ongoing crypto-market volatility. CEO Brian Armstrong was direct: to remain competitive, the exchange must become “AI-native.” Compliance, KYC and tier-one support are being reorganised into “AI-native pods” replacing legacy operations.
Firing the Coders and the Freelancers
Freshworks cut around 500 roles (eleven per cent) on 5 May. The CEO publicly noted that more than fifty per cent of the company’s code is now AI-generated. The remaining engineers’ AI tools are producing enough code to cover the spread.
Upwork slashed roughly 145 roles (twenty-four per cent) on 7 May. The premier platform for freelance human labour framed the cuts in terms of an “efficient operating model” and the “evolving nature of work.” It is not a clean AI-replacement admission. But the subtext is hard to miss: a platform whose entire business model is built on selling human hours has decided it needs fewer human hours of its own.
The Efficiency-and-Buyback Combo
BILL Holdings announced on 7 May that it is slashing up to thirty per cent of its workforce (up to 700 roles) and pairing the cuts with a one-billion-dollar share buyback. The market mechanic is brutally traditional: flatten the org chart, automate the residual workflows, return the payroll savings to shareholders.
Microsoft’s $900 Million Golden Handshake
The full details of Microsoft’s first-ever voluntary retirement programme emerged this week. Approximately 8,750 senior US employees are eligible. The company is taking an estimated $900 million charge. Eligible workers must hit the “Rule of 70” (age plus tenure) and receive a lump-sum severance, one year of subsidised healthcare with the option to continue for four more, and accelerated stock vesting.
This is a different category from the Cloudflare-style cuts. Microsoft is not telling its senior workforce that AI made them obsolete. It is reshaping the demographic profile of a 51-year-old company that has accumulated decades of long-tenure staff. The result is the same shape on the org chart, but the story is workforce reshaping rather than AI replacement.
Voluntary buyouts are quietly replacing mass layoffs across the corporate landscape. They sidestep WARN Act notices, they protect employer brand, and they allow workers to exit on their own terms. The headline reads “Microsoft offers retirement to senior workers” rather than “Microsoft cuts 8,000 jobs.” The optics matter as much as the maths.
High-Probability Targets: Week 21
Mid-Market SaaS and Cybersecurity. With Cloudflare setting a twenty per cent efficiency benchmark for infrastructure, expect intense pressure on Okta, CrowdStrike and Zendesk to announce comparable AI-native restructurings.
B2B Service Marketplaces. Upwork’s twenty-four per cent cut is a leading indicator. Any platform acting as a middleman for digital human labour (Fiverr, Toptal) is facing an existential threat from autonomous agents.
Final Thought
The pattern of every previous wave was the same. Institutions resisted. The technology moved anyway. Eventually the people who delayed the benefit became footnotes.
The fifth wave will move faster.
The FDA has moved first. Patients with smartphones are already moving second. The NHS has pilots, committees and funds, but not yet an operating model equal to the moment.
The clinicians who learn to direct AI will become the doctors of the next decade. Those who do not will not disappear, but they will be trapped inside a system built for an earlier age.
The MHRA does not have years to answer the FDA. It has months. Every delay now is not abstract. It means capital lost, trials lost and patients left waiting.
Two centuries fighting disease from the outside.
The next two, rewriting biology from within.
Those who build for the fifth wave will define the next century of medicine.
Those who wait will spend it explaining why.
🚀
Until next Sunday, David
The Sunday Signal is published weekly at thesundaysignal.ai. No hype. No hedging. Just the signal.